References
1. van Buul LW, van der Steen JT, Veenhuizen RB, Achterberg WP, Schellevis FG, Essink RT, et al. Antibiotic use and resistance in long term care facilities. J Am Med Dir Assoc. 2012;13(6):568. e1-568. e13.
2. Crnich CJ, Jump R, Trautner B, Sloane PD, Mody L. Optimizing Antibiotic Stewardship in Nursing Homes: A Narrative Review and Recommendations for Improvement. Drugs Aging. 2015 Sep 1;32(9):699–716.
3. Cassone M, Mody L. Colonization with Multidrug-Resistant Organisms in Nursing Homes: Scope, Importance, and Management. Curr Geriatr Rep. 2015 Mar 1;4(1):87–95.
4. Daneman N, Gruneir A, Bronskill SE, Newman A, Fischer HD, Rochon PA, et al. Prolonged antibiotic treatment in long-term care: role of the prescriber. JAMA Intern Med. 2013;173(8):673–82.
5. Fleming A, Bradley C, Cullinan S, Byrne S. Antibiotic Prescribing in Long-Term Care Facilities: A Meta-synthesis of Qualitative Research. Drugs Aging. 2015;32(4):295–303.
6. Daneman N, Bronskill SE, Gruneir A, Newman AM, Fischer HD, Rochon PA, et al. Variability in antibiotic use across nursing homes and the risk of antibiotic-related adverse outcomes for individual residents. JAMA Intern Med. 2015;175(8):1331–9.
7. Wu JH-C, Langford BJ, Daneman N, Friedrich JO, Garber G. Antimicrobial Stewardship Programs in Long-Term Care Settings: A Meta-Analysis and Systematic Review. J Am Geriatr Soc. 2019 Feb;67(2):392–9.
8. Barlam TF, Cosgrove SE, Abbo LM, Macdougall C, Schuetz AN, Septimus EJ, et al. Implementing an antibiotic stewardship program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;62(10):e51–77.
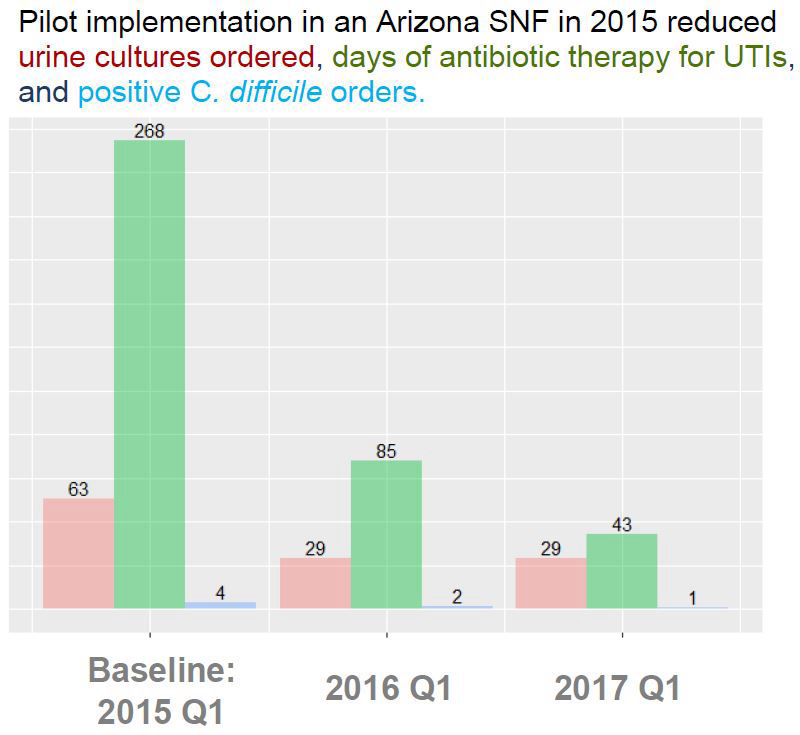
9. Patterson PP, Ellingson KD, Backus D, Schmitz E, Matesan M. A syndrome-based approach to antimicrobial stewardship in an Arizona skilled nursing facility-Moving the needle through quality improvement. Am J Infect Control. 2020 Dec;48(12):1537–9.
10. Jump RLP, Gaur S, Katz MJ, Crnich CJ, Dumyati G, Ashraf MS, et al. Template for an Antibiotic Stewardship Policy for Post-Acute and Long-Term Care Settings. J Am Med Dir Assoc. 2017 Nov 1;18(11):913–20.
11. Toolkits | Agency for Healthcare Research and Quality [Internet]. [cited 2021 Feb 24]. Available from: https://www.ahrq.gov/nhguide/toolkits.html
12. The Core Elements of Antibiotic Stewardship for Nursing Homes. :21.
13. LeGros T, Kelley C, Ellingson K. Barriers and Facilitators to Antibiotic Stewardship at Skilled Nursing Facilities Suggest a Systems Approach. Unpubl Manuscr. 2021;
14. Naughton BJ, Mylotte JM, Ramadan F, Karuza J, Priore RL. Antibiotic use, hospital admissions, and mortality before and after implementing guidelines for nursing home–acquired pneumonia. J Am Geriatr Soc. 2001;49(8):1020–4.
15. Szymczak JE, Feemster KA, Zaoutis TE, Gerber JS. Pediatrician Perceptions of an Outpatient Antimicrobial Stewardship Intervention. Infect Control Hosp Epidemiol. 2014 Oct;35(S3):S69–78.
16. Langford BJ, So M, Raybardhan S, Leung V, Soucy J-PR, Westwood D, et al. Antibiotic prescribing in patients with COVID-19: rapid review and meta-analysis. Clin Microbiol Infect [Internet]. 2021 Jan 5 [cited 2021 Feb 11]; Available from: https://www.sciencedirect.com/science/article/pii/S1198743X20307783
17. Rantz MJ, Zwygart-Stauffacher M, Flesner M, Hicks L, Mehr D, Russell T, et al. The Influence of Teams to Sustain Quality Improvement in Nursing Homes that “Need Improvement.” J Am Med Dir Assoc. 2013 Jan;14(1):48–52.
18. Bassetti M, Paiva J-A, Masterton RG. The case for de-escalation in antimicrobial therapy: time to change our strategy in the management of septic shock? Intensive Care Med. 2014 Feb;40(2):284–5.
19. Katz MJ, Gurses AP, Tamma PD, Cosgrove SE, Miller MA, Jump RLP. Implementing Antimicrobial Stewardship in Long-term Care Settings: An Integrative Review Using a Human Factors Approach. Clin Infect Dis Off Publ Infect Dis Soc Am. 2017 Dec 1;65(11):1943–51.
20. Centers for Medicaid Services. Available from: https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Internet-Only-Manuals-IOMs-Items/CMS1201984
21. Stone ND, Ashraf MS, Calder J, Crnich CJ, Crossley K, Drinka PJ, et al. Surveillance Definitions of Infections in Long-Term Care Facilities: Revisiting the McGeer Criteria. Infect Control Hosp Epidemiol Off J Soc Hosp Epidemiol Am. 2012 Oct;33(10):965–77.